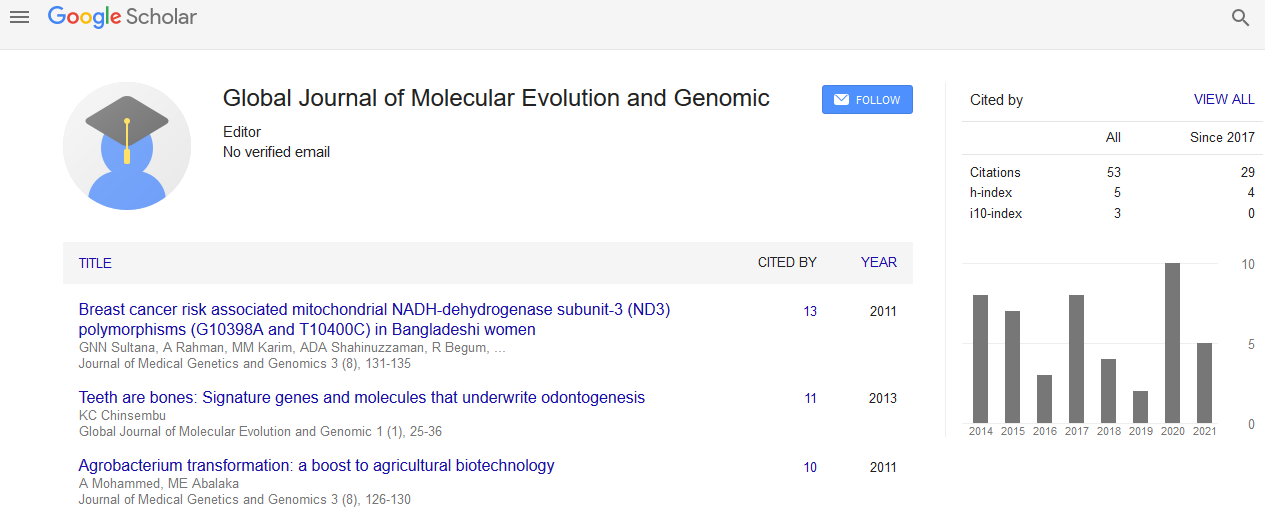
Global Journal of Molecular Evolution and Genomic received 67 citations as per Google Scholar report

Received: 01-Aug-2022, Manuscript No. GJMEG-22-73204; Editor assigned: 03-Aug-2022, Pre QC No. GJMEG-22-73204(PQ); Reviewed: 17-Aug-2022, QC No. GJMEG-22-73204; Revised: 24-Aug-2022, Manuscript No. GJMEG-22-73204(R); Published: 31-Aug-2022, DOI: 10.15651/GJMEG.22.08.010
A leading genital cancer, cervical cancer is thought to be the third most prevalent female gynecologic malignancy and the fourth most common cause of cancer death in women, with an estimated 570,000 new cases and 311,000 new deaths in 2018. (GLOBOCAN, 2018). Agestandardized cervical cancer incidence rates in poor nations are higher than those in wealthy nations (16.7 per 100,000 vs. 12.7 per 100,000 women-years, respectively). Around 14% of cervical cancer cases worldwide occur each year in China. As a result of rising cervical cancer morbidity and mortality in young women, China continues to deal with a relatively severe burden of managing public hygiene.
Cervical cancer has been linked mostly to the Human Papillomavirus (HPV), a sexually transmitted DNA virus from the Papovaviridae family. According to estimates, the majority of sexually active adults have at least one HPV Genotype. If the high-risk HPV infection persisted, cervical cancer may have a known aetiology if it were to develop. To present, more than 200 different HPV genotypes have been identified; of these, about 40 infect the mucosal epithelium of the mouth and genital tract. According to their known carcinogenic risk or potential pathogenicity, they are typically categorised as high-risk HPV (carcinogenic HPV types, HR-HPV), low-risk HPV (non-carcinogenic HPV types, LR-HPV), and intermediate-risk HPV (IR-HPV).
It's a well-known fact that this kind of cancer is one of the easiest to prevent. Currently, HPV vaccine and HPVbased screening programmes, which have been shown to successfully eliminate the burden of cervical cancer globally, are a part of comprehensive strategies targeted at controlling cervical cancer. However, because there are large variations in the prevalence and genotype distribution of HPV infections (both within and between countries and regions), making headway in prevention is frequently challenging. Therefore, it is crucial to have a precise understanding of the regional distribution characteristics of HPV genotypes for both the development of prophylactic vaccines based on HPV and the formulation of cervical cancer screening strategies based on HPV.
According to a global estimate of women, the prevalence of HPV was significantly greater in eastern Asia than in southeastern Asia and south-central Asia, where the rates were 13.6%, 6.2%, and 7.5%, respectively. Additionally, the HPV prevalence in less developed nations was higher than in more developed nations (10.0%), and eastern Asia has the highest HPV prevalence rates in the entire continent. The prevalence of HPV infection varies greatly among eastern Asian nations, with China bearing the most loads as the most populous emerging nation. Furthermore, it has been demonstrated that western China has the highest mortality rate and second-highest incidence rate of cervical cancer in China, making western China's primary cervical cancer prevention particularly crucial.
With frequencies of 19.93%, 14.52%, and 10.01%, the next three HR/IR-HPV types with the highest frequency were HPV16, 58, and 53. Our study's HPV distribution's features matched those of a recent finding in Guizhou, China. Contrary to our findings, a recent study with 37,722 female participants revealed that the most common genotypes were HPV 16 (3.79%), HPV 52 (2.47%), HPV 58 (1.76%), and HPV 53 (1.35%). Additionally, HPV16 (4.82%), HPV52 (4.52%), and HPV58 (2.74%) infection rates were all lower than those in our sample when compared to national data from a Chinese population-based inquiry from 37 cities, with the exception of HPV53 (not reported). Understanding the incidence of HPV and the distribution of its subtypes in various geographic areas may help with the design and execution of vaccination programmes.