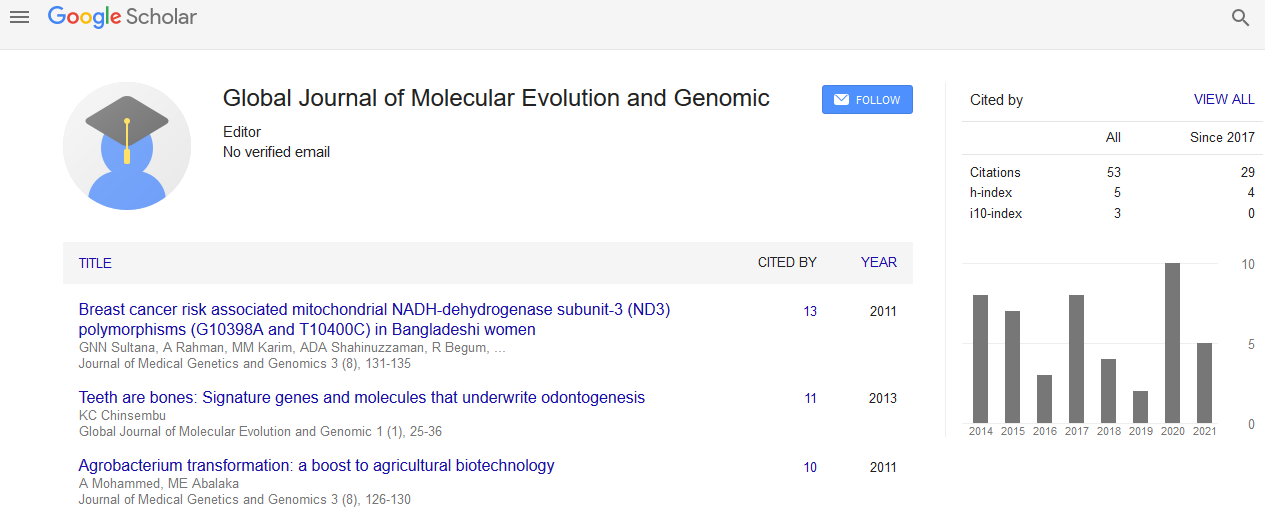
Global Journal of Molecular Evolution and Genomic received 67 citations as per Google Scholar report

Received: 01-Aug-2022, Manuscript No. GJMEG-22-73200; Editor assigned: 03-Aug-2022, Pre QC No. GJMEG-22-73200(PQ); Reviewed: 17-Aug-2022, QC No. GJMEG-22-73200; Revised: 24-Aug-2022, Manuscript No. GJMEG-22-73200(R); Published: 31-Aug-2022, DOI: 10.15651/GJMEG.22.08.007
Breast cancer has been the number one cause of death from malignant neoplasms in women for more than a decade. It primarily affects people in their fourth to sixth decades of life and affects people from all socioeconomic backgrounds. Over the past 50 years, the mortality rates for this neoplastic disease have significantly increased. In adult women of all age categories, the rate increased consistently between 1955 and 1960, hovering between two and four deaths per 100,000 women, although with a bigger impact on those over 30. According to the actual data, there are both modifiable and non-modifiable risk factors for breast cancer, making it a complex disease. The most significant modifiable factors are postmenopausal status, smoking, physical inactivity, and obesity. Approximately 10% of all incidences of breast cancer have been linked to inherited genetic autosomal mutations.
Breast cancer occurs more frequently in locations with greater socioeconomic earnings than in native communities where the socioeconomic level is lower, indicating significant regional disparities in incidence and prevalence. This data is consistent with the global epidemiology of breast cancer, which shows that affluent nations are affected more severely and that third-world populations have lower incidence and prevalence rates. More than a socioeconomic or environmental factor, some scholars have discussed the connection between various human societies' DNA, paying particular emphasis to the various mitochondrial haplogroups. The association of mitochondrial haplogroups with sporadic or familial hereditary breast cancer, however, has not been established.
The regulatory region D-loop of the mitochondrial DNA plays a significant role in the development of cancer because it contains crucial sequences for transcription and replication. These non-coding sections of the control region may contain polymorphisms that are significant in the development of breast cancer, according to earlier studies. These variations in the sequence can be linked to a certain phenotype and act as indicators for the emergence of different cancers. Different mitochondrial polymorphisms, however, appear to vary from population to population, according to some studies. Additionally, some polymorphisms have a stronger correlation with breast cancer than others.
Areas that are affected by polymorphisms are involved in the production of proteins and RNA for mitochondrial metabolism. The A10398G polymorphism, which is linked to the production of the protein NADH-ubiquinone oxidoreductase 3 (ND3), is one of the most frequently cited in literature and has been found to be a biomarker in a variety of populations, including Polish, Indian, Chinese, and primarily Afro-descendant groups. In populations of Asian descent, this polymorphism has also been linked to metabolic syndrome and mental health issues. However, when looking at this polymorphism alone, without associating with other mitochondrial polymorphisms in women affected by this malignancy, a meta-analysis found that there is no connection. Although the A10398G change increases the risk of breast cancer in Caucasian American human groups of European ancestry, additional polymorphisms with greater statistical significance have been found, such as the T16519C in the control region.
The many haplogroups linked to breast cancer resistance are unrelated to one another. However, when we looked at the sequence data, we could see polymorphisms that are frequently linked to breast cancer. It is significant to note that the majority of the samples are of European origin and that they share characteristics with the rCRS reference genome used in the database and genomic browsers as well as with 44.9% of the population who had breast cancer. Only nine of the 241 polymorphisms found exclusively in neoplastic tissue—A16183C repeat in 11 different sequences, T16217C in 5, and T16298C in 4 sequences—were repeated in more than three different sequences in our analysis. Some of these modifications to the mtDNA sequences have links to further malignant neoplastic disorders.
These D310 variations were found in 98% of the sequences examined. Although the majority of these polymorphisms are frequently linked to particular haplogroups, the 315.1C polymorphism was shown to be evolutionarily linked to the Indo-European haplogroup H and to have a frequency lower than 1.5%. 99% of the sequences of non-European origin were associated with breast cancer in our analysis.
T16519C and D130 polymorphisms are both evolutionarily connected to the Caucasian-originating haplogroup H, which has Indo-European and Euro-Asian ancestry. However, they were also discovered in all non- European sequences associated with breast cancer. Breast cancer patients' mtDNA alterations are polymorphic rather than linked to a few rare mutations.